A visual journey through orthopedic conditions. Discover the pathology in medical imaging, then in real life. A clear and focused perspective.
A bucket-handle tear is a severe longitudinal meniscal injury where the central fragment displaces into the intercondylar notch, often co-occurring with ACL tears. Frequently presenting as a locked knee, it is diagnosed on MRI via distinct signs like the "double PCL" and "absent bow-tie" before direct visualization and repair during arthroscopy.

Bucket-handle tear: a meniscal injury subtype
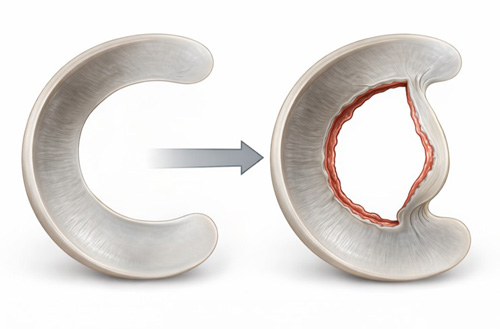
- Bucket-handle tears (BHT) are a specific subtype of longitudinal meniscal injury characterized by displacement of the central fragment toward the intercondylar notch.
- Accurate and timely diagnosis, based on preoperative MRI and confirmed by arthroscopic evaluation, is essential to guide appropriate management.
- Given the key biomechanical role of the meniscus, preserving viable tissue whenever possible remains crucial to maintain joint homeostasis and support long-term knee function.
Bucket-handle tear: a clinical point of view
- From a structural perspective, a longitudinal meniscal tear divides the tissue into two distinct components: a stable peripheral rim and an inner mobile fragment.
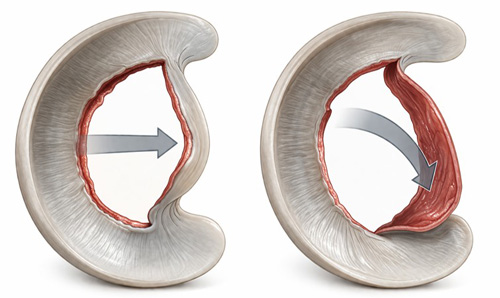
- As displacement occurs, the central fragment may migrate toward the intercondylar notch, where it can become entrapped, resulting in a mechanical obstruction of the joint.
- Clinically, this manifests as locking, catching, and palpable or audible clunks, often leading to functional limitation and loss of full knee extension.
Bucket-handle tear + ACL tear
- BHT are frequently associated with anterior cruciate ligament (ACL) injuries, particularly in acute traumatic settings. Rotational instability may contribute to both the occurrence and displacement of the lesion.
- Their presence can further compromise joint stability and influence surgical planning, making accurate diagnosis essential.
- Addressing both meniscal and ligamentous pathology is crucial to restore knee biomechanics and optimize outcomes.
- Magnetic resonance imaging (MRI) is highly effective in diagnosing bucket-handle meniscal tears, with reported sensitivity and specificity ranging from approximately 86% to 90%.
- The diagnosis is based on a combination of characteristic imaging findings that reflect both the disruption of normal meniscal morphology and the displacement of the torn fragment.
- Three key MRI signs include the absent bow-tie sign, the double PCL sign, and the presence of a displaced fragment within the intercondylar notch.
MRI coronal view – White arrows: displaced medial meniscal fragment within the intercondylar notch, associated with truncation and reduced size of the meniscal body.
MRI sagittal view – White arrows: double PCL sign, with a low-signal band paralleling the posterior cruciate ligament, representing a displaced meniscal fragment within the intercondylar notch.
MRI sagittal view – White arrows: double delta sign and absent bow-tie sign, indicating anteriorly displaced central meniscal fragment and absence of the normal meniscal body on sequential sagittal images.
MRI axial view - White arrow: the central fragment migrated toward the intercondylar notch.
Patient positioning for knee arthroscopy: the patient is placed supine with the operative leg positioned against a lateral post, allowing knee flexion and application of valgus stress to facilitate access to the medial compartment.

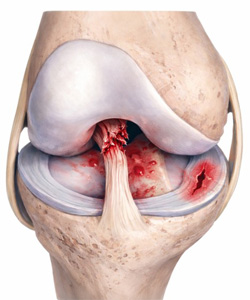
Anterior view of the medial compartment of the knee with the diagnosis of a bucket-handle tear of the medial meniscus.
Arthroscopic view reduction of the displaced meniscal flap using a probe, restoring its native position within the meniscal rim.
Arthroscopic view while tears in the red–red and red–white zones may be amenable to repair, lesions involving the white–white zone, as in this case, are typically managed with selective meniscectomy of the unstable flap and contouring of the remaining meniscal tissue.